Here’s our take on the recent American Academy of Pediatrics Clinical Report (not a guideline).
First, the good. They recommend exclusive breastfeeding for six months and two years or longer as mutually desired by the infant and mother. They also support a team approach to care (although it’s limited). They are bringing awareness to tongue-ties as a real medical issue, and as they say, “any publicity is good publicity.”
This AAP clinical report mirrors and doesn’t add anything that the ENT consensus statement (AAO-HNS) from 2020 stated that says tongue-ties are overdiagnosed, there’s no clear consensus, and tongue-ties rarely cause issues. I’m not sure why they spent the time to re-create it, but I think they had pressure from others in their organization to address the “fad” of tongue-tie treatment that pediatricians encounter in their office every. single. day.
The bad… they suggest that a tongue-tie can stretch out since there is genioglossus muscle inside it. With the CO2 laser, every time I release a tongue-tie it is essentially an in vivo dissection (as opposed to Mills’ cadaver dissection), and I can clearly see when it is primarily fascia, has some muscle fibers or the frenum is primarily muscle (often it’s extra aberrant muscle fibers and not the true genioglossus muscle). These are very thick, have a tented appearance, and are so restrictive the tongue goes nowhere. They certainly do not stretch out and can be observed in children and adults (been there for decades without stretching!). They cannot easily be treated with scissors due to the significant bleeding that would occur and loss of surgical field that would ensue.
The article says that less than 50% of infants with tongue-tie have feeding problems. It’s hard to know the true incidence because that statistic is likely referring to restrictions that are at or near the tip. We observe this clinically, with some families coming to see us for a consultation with a to-the-tip 100% tongue restriction but with few symptoms. The baby is gaining weight, and the mother is not in pain. These are the two criteria that pediatricians and primary care providers most often assess as to the necessity of release.
So in that sense, yes, there is a subset of infants who feed asymptomatically with these two narrow parameters. When you look at the broader implications of a restricted tongue and seal issues like aerophagia which leads to reflux, colic, gas, spitting up, milk leakage, nasal congestion, as well as the potential for future issues of speech, solid feeding, sleep, dental development, mouth breathing, etc. then a holistic evaluation is needed. To diagnose well and certainly not over-treat, but also not under-treat, it requires obtaining a full history, comprehensive examination, and thorough discussion with the parents before you determine if the tongue restriction is “asymptomatic” and does not need treatment.
Imagine if a child had syndactyly where the fingers were literally stuck together, would we leave that child to compensate and not offer a fix in early childhood? We don’t know if they will want to be a concert pianist later in life, but it’s fixed because it’s on the hand and obvious to anyone that passes by that this can affect handwriting, eating, sports, typing, etc. Who wants their child to be limited or held back by a physical condition that can be easily remedied? Why do we then leave the tongue alone when it has even more important bodily functions than just webbed fingers, and it has been clearly seen that it does not self-correct and can cause a lifetime of issues?
Throughout the “evidence-based” clinical report, they fail to evaluate and cite Dr. Ghaheri’s randomized-controlled trial on bottle-feeding (and breastfeeding) babies that showed objective feeding improvements after releasing only posterior (not obvious) tongue-ties. This was a glaring and obvious censorship move because it did not agree with their narrative. The term posterior tongue-tie is not the best term, as in the report they mistakenly think it means the posterior part of the tongue is held down. In fact, it’s the middle portion of the tongue, so a better term is “mid-tongue restriction” but it’s simply referring to a frenum that is not to the tip, but less than 50% to the tip, or posterior to the salivary ducts, but in the same place you would expect the frenum to be.
Throughout the rest of the report they drop hints that there is over-diagnosis, people are just doing the procedure for the money, and the dentist needs to defer to the pediatrician essentially. They sadly mention many rare but serious conditions to check before saying that a feeding problem could be from tongue-tie like heart disease, inborn errors of metabolism, or intestinal obstruction. Inborn errors of metabolism like PKU 1 in 10,000 babies, or GAMT is 1 in 250,000, so a pediatrician is unlikely to ever see that in practice. Meanwhile, tongue-tie is estimated at 25% (and some studies say as high as 32.5%) so it is likely that every single day a pediatrician will have a child or baby who is suffering from an undiagnosed tongue-tie.
What happens to these babies? Symptomatic relief (band-aids): gas drops, gripe water, rice in the formula, prune juice for constipation, reflux medicine, nipple shields, bottles and formula.
Later, they say that there are no studies or insufficient evidence to point to using a laser. I know of one study, Haytac 2006, published in a good journal, that looked at scalpel (blade) vs. CO2 laser and had favorable results for the laser. So they left that one out. But do we need a study that says that it is easier to do complicated math problems with a calculator than by writing it out by hand? Do we need a study that it is superior or faster to drive in a car than to walk or ride a bicycle? How about the authors try both methods and then determine which is easier and superior and gives better results?
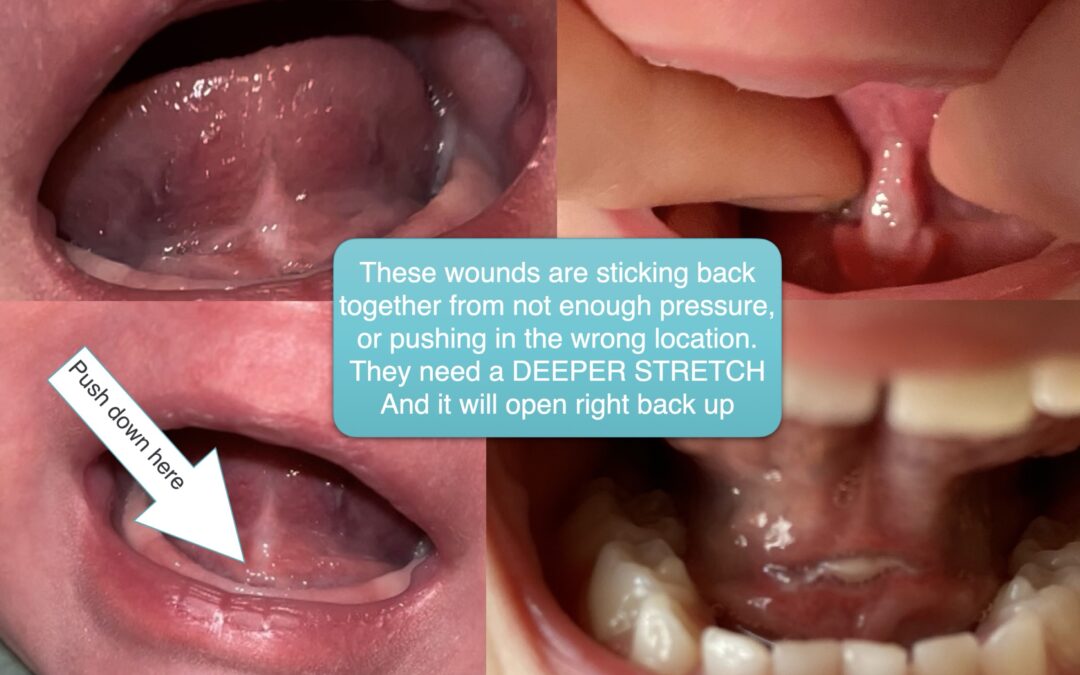
They advocate for a team approach, but not including physical therapists, chiropractors, CST, myofunctional therapists, etc. They also say stretches aren’t needed. If your ear is pierced, and you don’t wear the earring, it will close back up. If you do a full release, and have a diamond-shaped wound, then it will close back up (possibly tighter) if stretches are not performed. We do not need a RCT on this fact. Patients come back and tell us they couldn’t do the stretches because the child or family was sick, and it grew back together. I stretch it, and it opens back up and restores the function of the tongue. It’s just like we don’t need a study to say that when you take out an infected tooth, the pain will go away. Some things are just clinically obvious to those providers who are doing this every day.
Speaking of research, they mention that they want randomized-controlled trials of lip-ties, tongue-ties, etc. This is nearly impossible to do in private practice, and no medical centers are wanting to do this research, so they know that it is not going to happen and it allows them to continue to say that treating tongue-ties don’t work. In many cases, it’s actually unethical and unreasonable to tell a parent “your child has a tongue and a lip-tie, but today we are going to treat just the lip-tie for a study to see what happens.” No one would agree to that (I’ve asked parents just to see what they would say, and they look at me like I’m crazy). So that’s not going to happen. So we have to just use our best judgment, clinical experience, and judiciously treat lip or cheek ties, trying not to under or over-treat, and offering the best care we can to the patients that are in our care today.
That’s where the clinical report falls short. What should the pediatrician do with these babies who have tongue-ties? The report doesn’t say. It just says there’s not enough evidence, try to work with a team approach, consider other super rare conditions before considering the most likely explanation. Remember Occam’s Razor, that the simplest explanation that fits the criteria is most often the right choice. If an infant has feeding issues, they should assume it’s a tongue-tie and rule that out first, before diving down the rabbit hole of other rare possible excuses and get that family help from a knowledgable provider with experience in diagnosis and treatment.
If you are a provider looking to learn more, we have courses at TongueTie.com/Professionals, we have all of our forms we use to help assess for tongue-ties on the site too for a free download on the Professionals page. We also have our multi-disciplinary book Tongue-Tied which explains all of this in detail. We donate all the profits from the courses and book to charity. We’re just trying to spread awareness and education of the topic.
If you’re a patient looking for answers, or for an evaluation for your child, just send us a message or take the quiz. Or just give us a call at 205-419-4333 and we would love to help you and your family.