This is a complex topic with many varied approaches and strong opinions with little to no research on the topic. It is a difficult topic to standardize and research, and we have gone through variations in what we recommend to parents concerning stretching duration, frequency, and technique. Below is our current technique based on treating over 10,000 tongue-ties in the past and refining our techniques continually based on follow-up observations.
Why Stretch?
First, why do we need to do wound care in the first place? Suppose a frenotomy or a clip or snip is performed (typically an ENT, pediatrician, or at the hospital). In that case, a small line wound is present, which is unlikely to reattach because the tongue is still restricted. A clip or snip can help with a few issues (perhaps nursing pain), but to see the full resolution of symptoms that most parents desire, you need: 1. a complete evaluation, 2. a full release of all restricted tissues, 3. appropriate wound care (discussed below), and 4. follow-up with a team approach for best results. In many ways, doing proper stretches is just as important as the procedure!
What’s a Full Release?
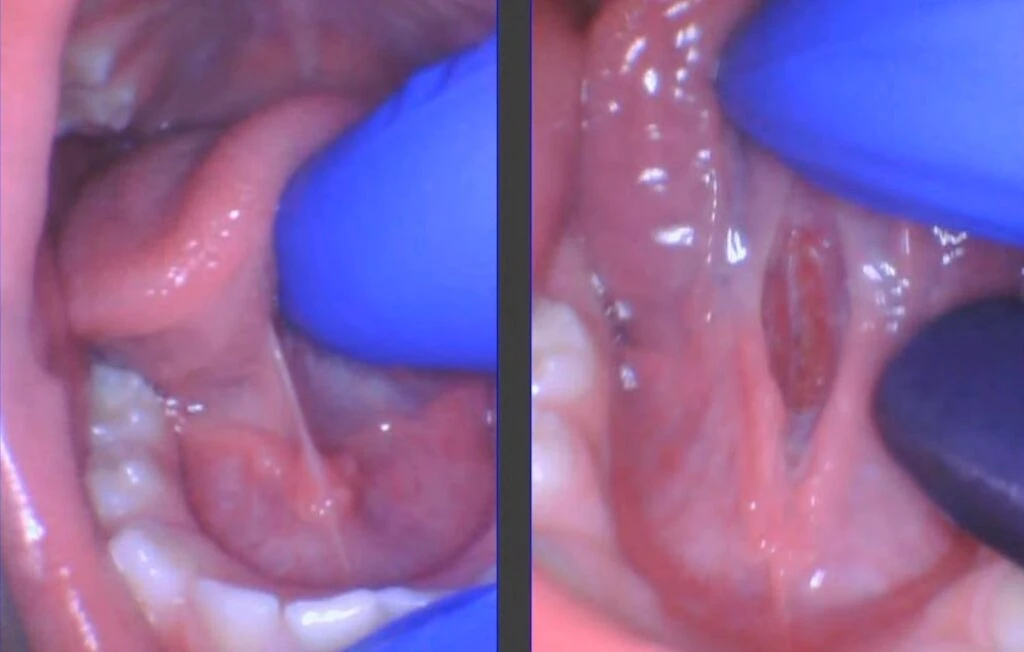
When we perform a full release, we remove all the restricted tissue down to the genioglossus muscle. It is possible to do this with scissors, a diode laser, and an erbium laser, but we prefer the CO2 laser due to its blend of cutting efficiency and minimal bleeding during the procedure. With the CO2, we can have the best visual and tactile access to the release area. A typical release takes just seconds and can provide the patient with full mobility of the lip, tongue, or cheeks. With a better range of motion and unhindered function, the patient now can breastfeed, bottle-feed, speak, eat, sleep, or breathe easier – they just need to re-learn (and that’s where the team approach helps with various therapists and modalities depending on the age and presenting symptoms).
Reattachment
With all of that out of the way, here are the specifics. We have to prevent the wound from readhering, also called reattaching. If you had your ear pierced but didn’t wear the earring, it would close up, and you would need to be pierced again. It’s the same with the tongue-tie release (lip-tie, cheek-tie, etc.). You have to do stretches or the wound edges will stick back together – end of story. People who say you don’t need stretches are performing a minimal clip, are inexperienced, or do not have patients back for follow-up and see how much tissue grew back together. Even if the wound is sutured, stretches are still needed, as sutures fall out within 3-7 days typically, and the wound readheres below the sutured area.

Babies
For infants, we recommend stretches 3 times a day for 4 weeks starting the day after the procedure. Three times a day is the most often you can reasonably expect parents to do with high-quality stretches. Four weeks is the typical duration of the wound contraction phase of wound healing. Some take longer and may need 6 weeks. Often the lip is healed at 3 weeks. We say 4 weeks, which prevents reattachment in more than 99% of patients (our reattachment rate needing a second procedure is less than 1%). We start the next day to give the parents and child a break.
Kids
For children, we recommend 2 times a day, for 4 weeks, starting the day after the procedure. Babies heal faster than children (12 months and up is when we switch to 2x a day). For a toddler, the most you can reasonably expect a parent to do stretches is twice a day.
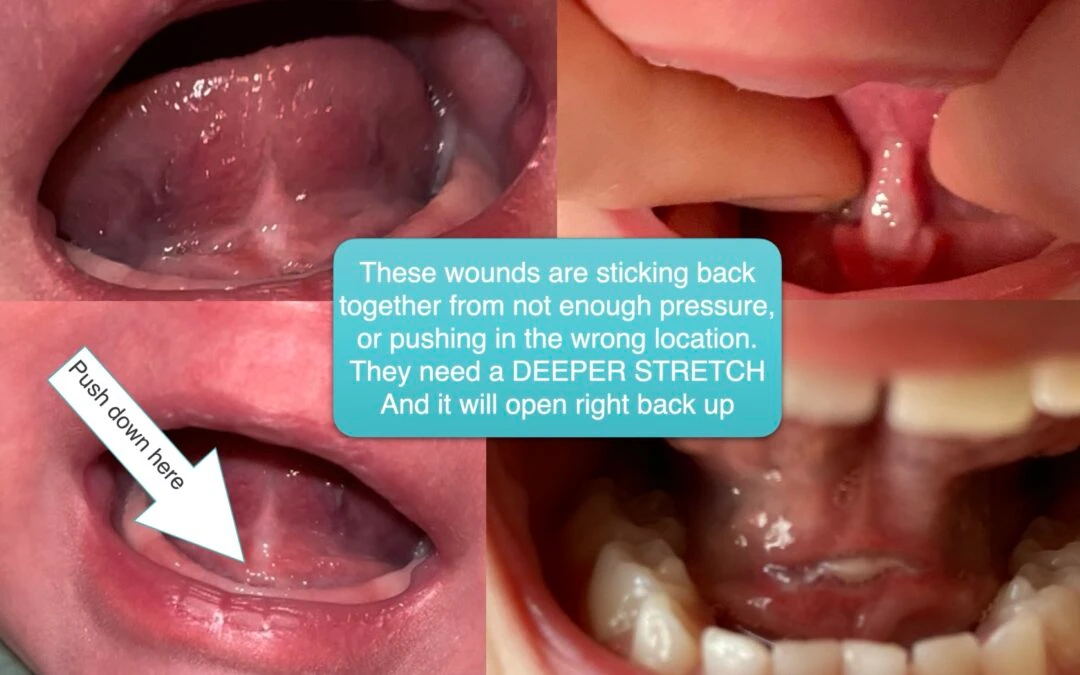
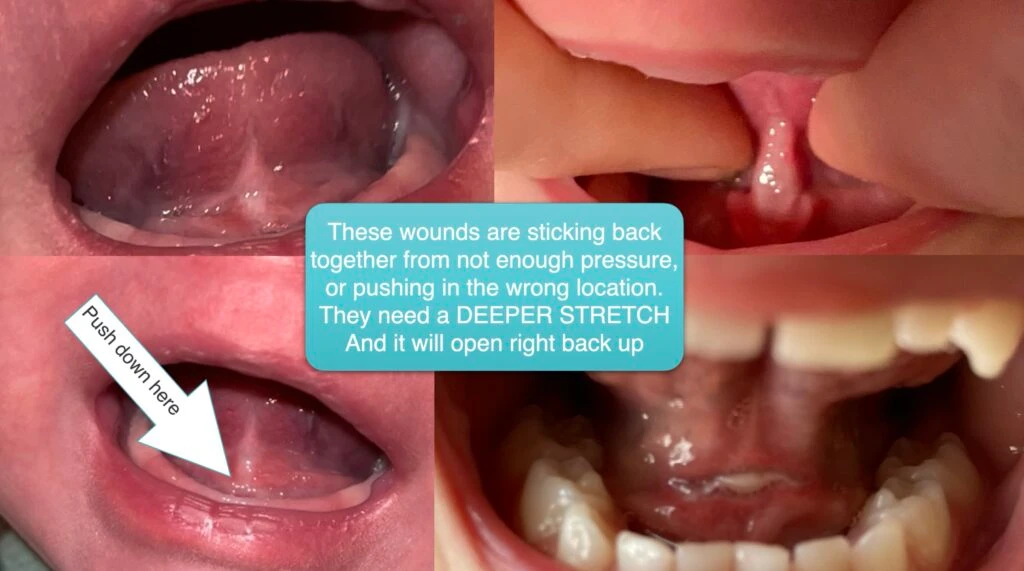
For the technique, you have to put firm pressure on the wound, like you were massaging someone’s back. Without sufficient pressure, the massages will not encourage the tissue to stop sticking back together. When we see the beginning signs of reattachment at the one-week follow up (90% are partially sticking back together even with stretches), parents are often not pushing with enough pressure or not pushing slowly and with pressure right in the middle of the scab and visualizing the diamond shape. At the follow-up visit, we demonstrate a stretch in the office again. We call it a “deeper stretch,” but it’s just a standard stretch. And the wound will often reopen with moderate pressure if done with the correct technique.
Technique
For infants and kids, use your non-dominant thumb to hold their jaw down to prevent them from biting or closing and limiting access to the area under the tongue. For kids with back teeth, we give parents an adjustable Molt mouth prop or “tooth chair” so they can effectively do stretches without losing a finger. So hold the jaw down on babies, or use the tooth chair (see photo). Cradle the head with both hands and come from behind with the baby lying on a changing table or sitting in the other parent’s lap, laid back into the parent’s lap who will stretch it (knee to knee position).

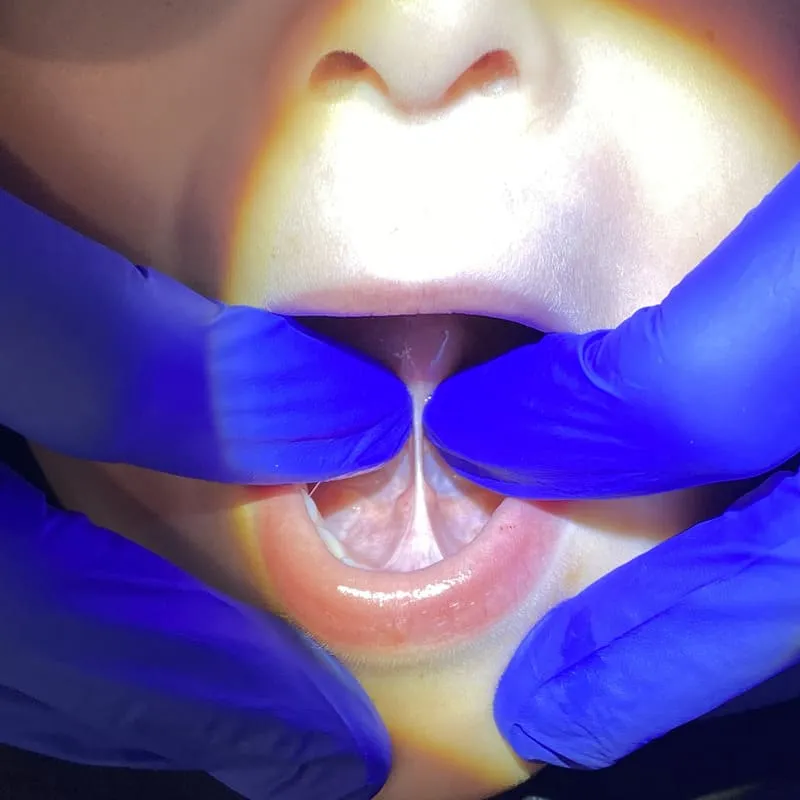
Push with the dominant hand’s index finger straight down behind the gum pad (or lower teeth if present), with the pad of the finger into the floor of the mouth. You have to work your way into the area under the tongue sometimes. Push down into the floor of the mouth, and as you are pushing down, SLOWLY scoop and slide the finger back (as you are still pushing down). You have to maintain pressure as your finger rides back and up the wound to elongate or stretch it out. You should wear a headlamp to see well; gloves make it easier, too. It’s like doing a Heimlich maneuver, scooping ice cream, or imagining a skateboarder on a half-pipe. Just push down. As you go down, keep pushing down slowly, and take your finger up the undersurface of the tongue and then hold it for around 5 seconds to see the diamond elongate.

All you are trying to do is elongate the wound so it’s not sticking back together. If it does stick back, you will see a horizontal line where it sticks back (it first sticks together in the middle of the diamond). Or it will look like a thicker area with less tongue mobility (see photo).
What if it Sticks Back Together?
If the tongue sticks back together, as long as it’s been within a few weeks, a more firm, slow stretch can help it to open back up, and it does NOT need to be lased again. This is a common mistake among newer providers. First, the release provider should try a stretch before performing a second procedure (revision) with the laser. If after pushing on it and no movement or reopening occurs, then a better option to restore function is to laser it again. But stretches must be done with more pressure, an additional follow-up visit (or two), and three more weeks of stretches will be needed. Something must be changed since the first release, or the wound will readhere again – the definition of insanity -doing the same thing and expecting a different result.

Here’s a video from our YouTube Channel on infant stretching and child/teen/adult stretching.
If your baby, child, or you had a tongue- or lip-tie release and you are worried it reattached, contact the provider or if we did it, please message us or call us and we would be happy to guide you through it. If you had your child’s procedure elsewhere and are concerned it grew back together and symptoms returned or never improved, please give us a call or message us and we can schedule a consultation for a possible revision. We have many people travel to see us from around the country and even other countries to have it revised for a second or third time due to an incomplete release, not being told to do stretches, or ineffective stretches. We would be happy to help you out.
Providers looking to learn more? Check out our Tongue-Tied Academy courses that go over all these details and more in easy-to-digest video lessons.